
The information contained in this article is for educational and informational purposes only and is not intended as health or medical advice. Always consult a physician or other qualified health provider regarding any questions you may have about medical conditions or health objectives.
Authors: Nick (Wear Tested Gear Review) & Dr. Mark Cucuzzella (NRC)
This article was originally published on Wear Tested – Gear Review & Healthy Aging.
TLDR;
Your cardiorespiratory fitness – how well your heart and lungs perform under effort – is one of the strongest predictors of how long you’ll live, stronger even than smoking, diabetes, or high blood pressure. Scientists measure it using METs, a simple unit comparing exercise effort to rest. Studies tracking millions of people found that the least-fit individuals face a mortality risk four times higher than the fittest. The good news: gaining even one MET – roughly adding a brisk 30-minute walk most days – cuts your risk by around 13–15%.
Table of Contents
- Part One: What Cardiorespiratory Fitness Actually Means
- Part Two: What The Research Actually Found
- Part Three: What One MET Actually Looks Like In Your Life
- Part Four: You Don’t Even Need To Run A Treadmill Test
- Part Five: Why This Matters And What To Do About It
- Take Action: Exercise Is Not Just Prevention. It Is Treatment.
Forget cholesterol panels and blood pressure cuffs. Researchers tracking millions of people have found that a simple measure of how hard your body works during exercise – your METs – may be the most powerful mortality predictor we have.
There is a number your body knows intimately, even if you have never heard of it. It is not your blood pressure, your resting heart rate, or your cholesterol level – though doctors love to check all of those. It is a measure of how efficiently your heart, lungs, and muscles work together when you ask them to move you through the world. Scientists call it cardiorespiratory fitness, or CRF. And a wave of landmark research, tracking millions of people across decades, has found that it predicts how long you will live more reliably than almost any other health marker we know of.

The best part? You do not need a laboratory to understand it. You do not even need to strap on a breathing mask. In many of the most significant studies conducted between 2020 and 2026, researchers never measured oxygen directly at all. Instead, they used a straightforward unit called the MET – the metabolic equivalent of task – to capture how hard a body is working relative to rest. And what they found should change how every one of us thinks about fitness.
PART ONE: What Cardiorespiratory Fitness Actually Means
Cardiorespiratory fitness is not the same as being good at a sport, having strong muscles, or maintaining a low body weight – though all of those can influence it. It is specifically about how well your body delivers and uses oxygen while you are moving. Think of it as the engine displacement of your biological vehicle: a higher-CRF body can sustain more demanding activity for longer before running out of fuel.
The traditional gold-standard measure is VO₂ max – the maximum volume of oxygen your body can consume per minute during peak exercise, expressed in milliliters per kilogram of body weight per minute. Elite endurance athletes can achieve VO₂ max values above 70 or 80. A sedentary middle-aged person might sit somewhere between 25 and 35. Measuring it properly requires a laboratory, a treadmill, a breathing mask, and a technician. It is accurate. It is also impractical for most people on the planet.
This is where METs enter the story – and why they matter so much for understanding the research.
What is a MET?
The resting body as a baseline
One MET – one metabolic equivalent of task – is defined as the energy your body uses when you are sitting perfectly still. Technically, that is about 3.5 milliliters of oxygen per kilogram of body weight per minute. It is your metabolic idle speed.
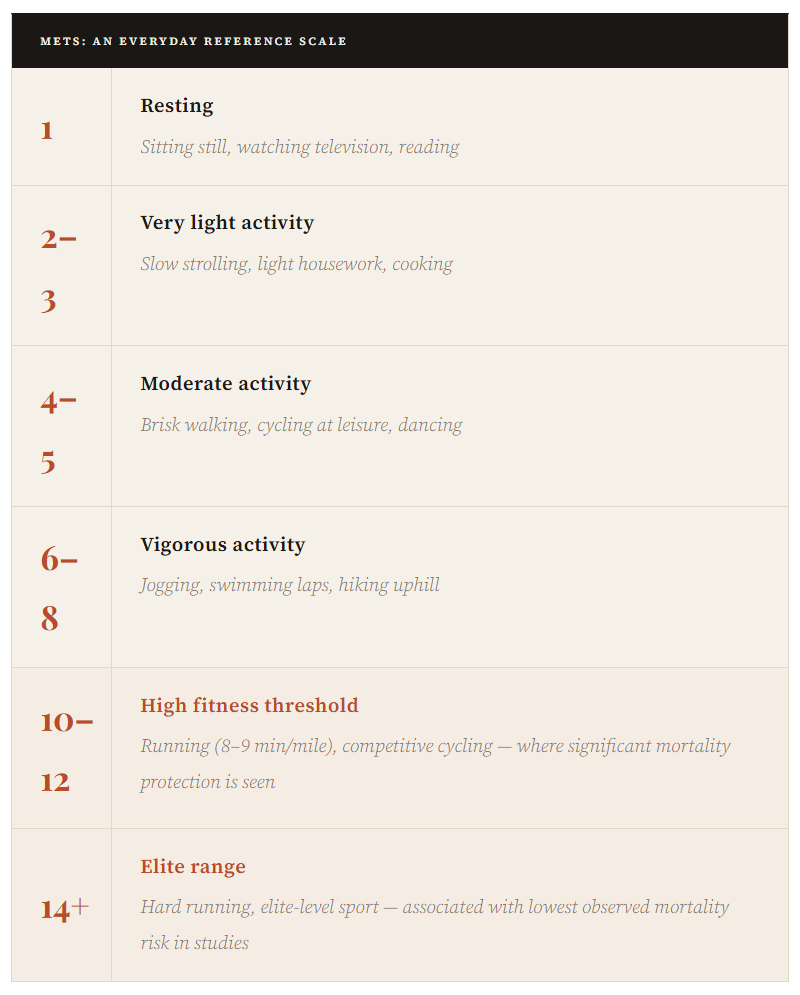
Every activity you perform is then expressed as a multiple of that baseline. Slow walking might be 2–3 METs. A brisk walk is around 4–5 METs. Jogging climbs to 7–8 METs. Running hard pushes above 10 METs. Cycling uphill or swimming fast might reach 12–14 METs. And truly elite athletes – pushing at maximum capacity – can sustain 18 METs or more.
The elegance of METs is that they are universal. A 140-pound woman and a 220-pound man will burn different total calories during the same activity, but their MET value – how many times their resting metabolic rate they are working at – is the same. That makes METs a powerful tool for comparing fitness and effort across different bodies, ages, and studies.
When doctors and researchers talk about “peak METs,” they usually mean the highest MET level you achieved during a maximal exercise test – walking on a treadmill that gets progressively steeper and faster until you cannot continue. That number, it turns out, is remarkably good at predicting what is going to happen to your health.

PART TWO: What The Research Actually Found
Between 2020 and 2026, several large studies converged on findings so consistent and so striking that even researchers who have spent careers in the field describe them as extraordinary. The numbers involved are not small: we are talking about studies tracking hundreds of thousands of – in some cases, millions – people over many years.
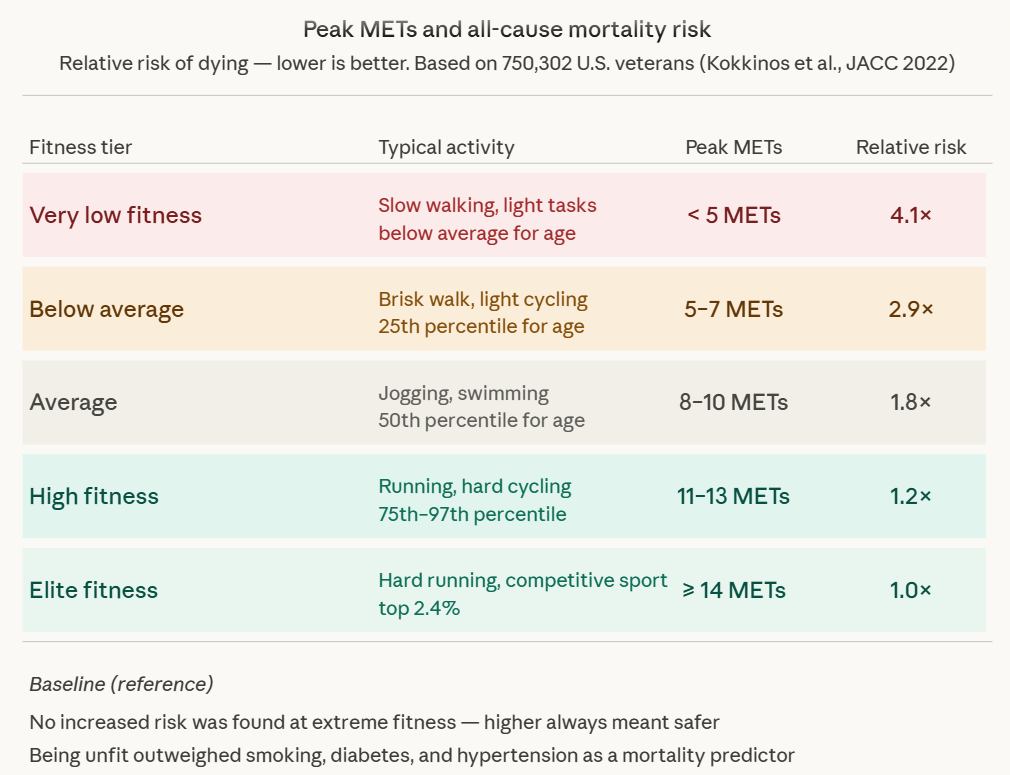
In 2022, a team led by researcher Peter Kokkinos published what became one of the most-cited fitness studies of the decade. Using data from 750,302 United States military veterans – men and women, ages 30 to 95, spanning every major racial group – they tracked peak METs achieved on a standard treadmill test, then followed participants to see who lived and who died. The results were startling in their clarity: fitness was inversely, independently, and gradually associated with mortality across every group studied. The least fit people – those in the lowest fifth of performance – faced a risk of death more than four times higher than those who were extremely fit. And “extremely fit” was defined not as marathon-runner territory, but as achieving around 14 METs – something a fit 60-year-old can accomplish with dedicated training.
Equally important: no upper limit was found. The idea that you can exercise “too much” and increase your mortality risk – sometimes floated in popular media – was not supported. The fitter you were the better your survival odds. Every step up the ladder counted.
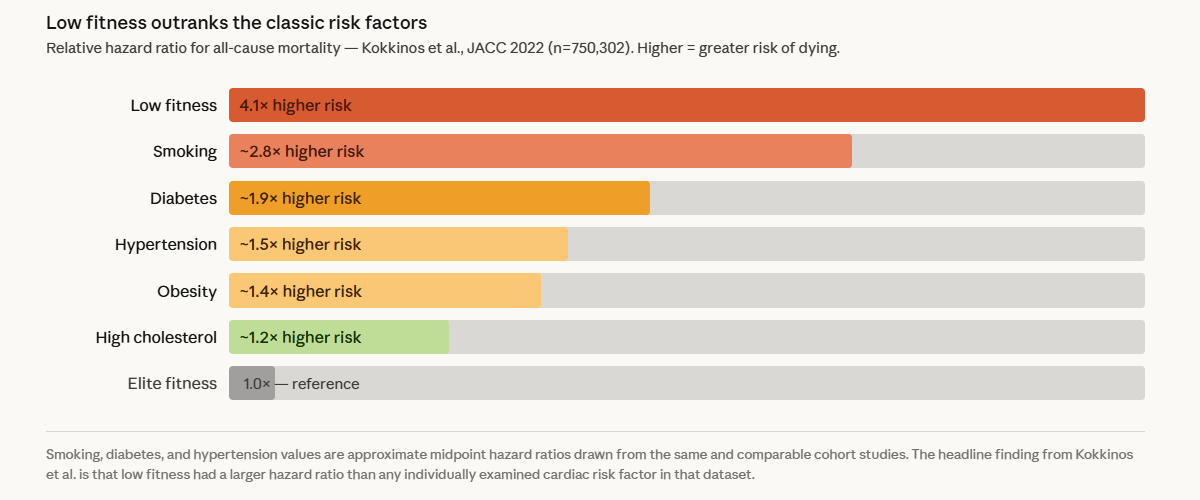
“Being unfit carried a greater risk than any of the cardiac risk factors examined.”
– Kokkinos et al., Journal of the American College of Cardiology, 2022
That is not a subtle finding. It means that in a head-to-head comparison, low cardiorespiratory fitness was a more powerful predictor of dying than hypertension, diabetes, high cholesterol, or a history of cardiovascular disease. This does not mean the other risk factors are unimportant – they absolutely are. But it does mean that fitness belongs at the top of the list, not buried as an afterthought.
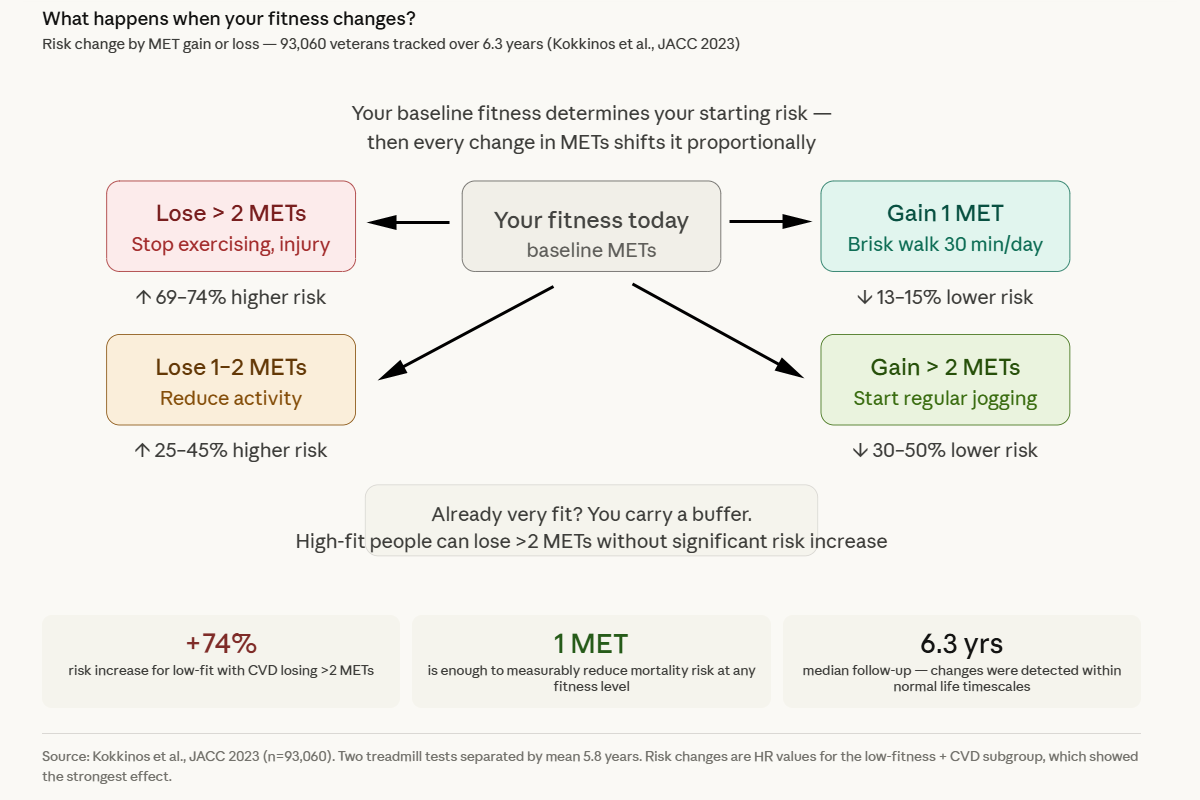
The 2023 follow-up study from the same Kokkinos team tackled a question that the original could not answer: what happens when your fitness changes? By studying 93,000 veterans who completed two treadmill tests separated by an average of nearly six years, they were able to show that changes in fitness produce proportional changes in mortality risk – in both directions. Gain a MET, your risk drops. Lose a MET, your risk rises. The relationship is almost mechanical in its precision.
One genuinely hopeful finding from that study: people who were already very fit seemed to carry a protective “buffer.” If you have built yourself up to a high level of fitness, a temporary setback – illness, injury, a period of inactivity – does not immediately erase your advantage. Your body retains something of what it has earned.
The mortality risk ladder – how your peak METs maps to survival odds.
It shows the five fitness tiers from very low to elite, their typical activity equivalents, and how mortality risk collapses from 4.1× down to 1.0× as you climb.
The fitness change clock – visualizing the 2023 finding that gaining or losing just 1–2 METs produces immediate, proportional changes in mortality risk.
It shows that risk tracks changes in fitness, not just the baseline. Losing two METs spikes your risk by 74%, gaining even one MET cuts it by 13–15%. The “buffer” finding for already-fit people is also shown.
PART THREE: What One MET Actually Looks Like In Your Life
All of this data becomes more useful when you can translate it into something tangible. What does “gaining one MET” actually require?
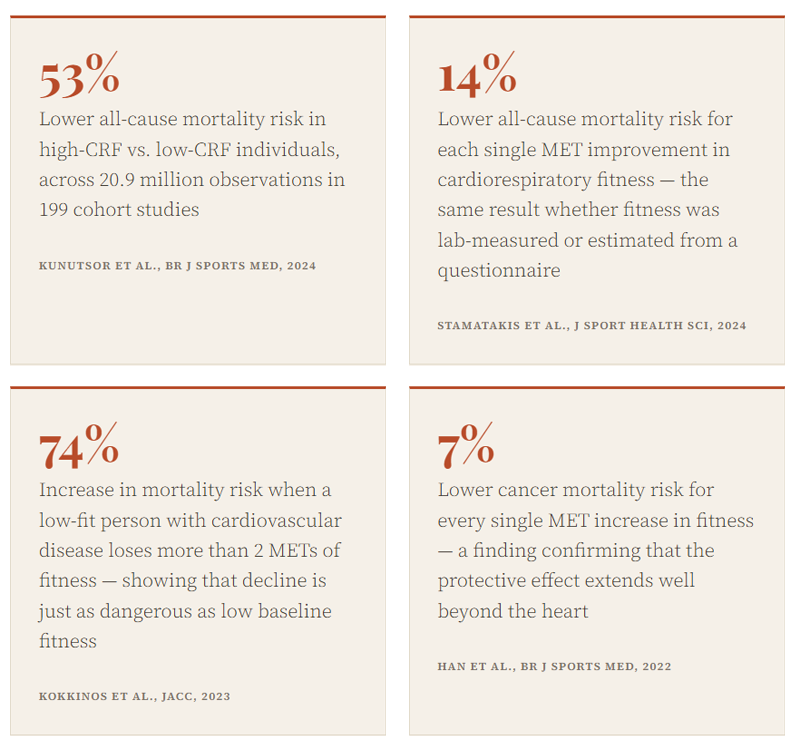
The research suggests that most adults who begin a moderate-to-vigorous aerobic exercise program can improve their peak MET capacity by one to two METs. That is not climbing Everest – that is walking briskly for 30 minutes most days of the week. It is adding a few jogs to your week. It is consistently choosing the stairs. And that one MET improvement is associated, in the research, with roughly a 13 to 15 percent reduction in the risk of dying.
The threshold of 7.9 METs has historically been highlighted in the research as a meaningful marker – people who can sustain activity at that level or above have substantially lower mortality rates than those who cannot. For a 50-year-old, that roughly corresponds to being able to jog without stopping. Not fast, not far – just consistently and without distress. That is not an impossible bar for most reasonably healthy adults to aim for.
CRF vs. other risk factors – putting low fitness in context by comparing it to the classic killers tracked in cardiology.
The bar chart that makes the key claim visceral: low fitness has a bigger hazard ratio than smoking, diabetes, hypertension, and high cholesterol combined in the same dataset.
PART FOUR: You Don’t Even Need To Run A Treadmill Test
One of the most consequential findings in recent fitness research is both quiet and radical: you do not need to step onto a treadmill to get a meaningful estimate of your cardiorespiratory fitness.
A 2022 study published in the European Journal of Preventive Cardiology took data from 330,769 people enrolled in the NIH-AARP Diet and Health Study and estimated their cardiorespiratory fitness using nothing more than a simple equation based on age, sex, body weight, height, and self-reported physical activity level. No exercise test. No laboratory. Just a questionnaire. Then they followed those people for nearly 15 years.
The result: that estimated fitness score – expressed in METs – predicted all-cause mortality, cardiovascular mortality, and cancer mortality with striking accuracy. People in the highest fitness quartile had roughly 35 to 40 percent lower mortality risk than those in the lowest quartile. And a sweeping 2024 meta-analysis confirmed the same finding across 42 studies and 3.8 million adults: the protective effect of fitness was equally strong whether it was measured with gold-standard laboratory equipment or estimated from a questionnaire, exercise-predicted, or calculated from everyday data.
The implication is significant. It means that cardiorespiratory fitness – as measured in METs – is ready to be used as a routine clinical vital sign, much like blood pressure or heart rate. Your doctor does not need a special machine. They need to ask you a few questions about how active you are, and they can get a reliable signal about your mortality risk.

PART FIVE: Why This Matters And What To Do About It
The sheer scale of the evidence accumulated between 2020 and 2026 – tens of millions of observations, consistent findings across age groups, sexes, races, and continents – means this is no longer a fringe hypothesis or a preliminary signal. Cardiorespiratory fitness is one of the most powerful modifiable predictors of how long a human being lives. And METs are its most accessible language.
The word “modifiable” is crucial here. Unlike your age, your genetics, or your family history, your cardiorespiratory fitness can be changed. It responds to training. It improves with consistent aerobic effort. And the research suggests the returns are not reserved for the already athletic: the steepest reduction in mortality risk occurs at the low end of the scale, moving from sedentary to moderately active. The person who goes from doing nothing to walking briskly for 30 minutes most days gains more, proportionally, than the person who moves from running a 10K to running a half-marathon.
“It really doesn’t take a whole lot to reap the benefits of exercise.”
– Peter Kokkinos, PhD, Washington DC Veterans Affairs Medical Center
The research also offers a message for the already fit: the buffer is real, but it is not infinite. Maintaining your fitness matters. A significant decline – losing two or more METs – is associated with a meaningful rise in mortality risk even for people who were once very fit. The body does not bank fitness the way a savings account accrues interest. It requires continued deposits.
What science does not prescribe is any single path. Walking, jogging, cycling, swimming, dancing, hiking – anything that raises your heart rate and keeps it elevated for sustained periods will build cardiorespiratory fitness. The optimal dose, according to current guidelines, is at least 150 to 300 minutes per week of moderate-intensity activity (roughly 4 to 5 METs, or a brisk walk), or 75 to 150 minutes of vigorous activity (7 METs and above). But even falling short of those targets produces measurable benefits compared to doing nothing at all.
The number your body knows is not a secret. It is being computed, moment by moment, every time you climb a flight of stairs, walk to the post box, or push a little harder on your weekend run. The question is whether we choose to pay attention to it – and whether, armed with what the research now shows, we give it the significance it deserves.
TAKE ACTION: Exercise Is Not Just Prevention. It Is Treatment.
The strongest argument for exercise is not that it helps healthy people stay healthy. That is true, but it understates the case.
The deeper argument is this: exercise is one of the few interventions that improves both quality of life and survival across many of the diseases that actually kill people.
No single medication, screening test, supplement, or procedure has this broad a reach. Statins help selected cardiovascular risk groups. Blood pressure medications reduce cardiovascular events when blood pressure is high. Cancer screening can detect certain cancers earlier. These are important tools. But each tool usually acts on one pathway, one disease category, or one risk group.
Exercise acts everywhere.
It improves endothelial function, insulin sensitivity, blood pressure, autonomic tone, skeletal muscle function, mitochondrial health, inflammation, mood, sleep, balance, frailty risk, and functional reserve. It changes the terrain on which disease occurs.
That is why the evidence becomes so compelling when we look at people who already have serious diseases.
Coronary artery disease: the clearest mortality signal
Among patients with coronary artery disease, exercise-based cardiac rehabilitation shows some of the strongest evidence for mortality benefit.
The evidence document summarized that exercise-based rehabilitation has been associated with a 36% to 63% reduction in total mortality in patients with coronary artery disease, and a 2023 meta-analysis of 85 randomized trials involving 23,430 participants found a 26% reduction in cardiovascular mortality, with a number needed to treat of 37.
The dose-response relationship is especially important. In the STABILITY study of 15,486 patients with stable coronary artery disease, exercise volumes of 10 to 20 MET-hours per week were associated with a 50% reduction in cardiovascular events. That is not an extreme training load. It is roughly the range achieved by regular brisk walking, cycling, or other moderate activity accumulated across the week.
The people at highest cardiovascular risk, including older adults, smokers, and those with diabetes or peripheral artery disease, often appear to benefit the most. In other words, exercise is not reserved for the young, lean, or already healthy. It may be most valuable for the people who are most vulnerable.
Heart failure: quality of life first, possible survival benefit
Heart failure is more complex. Randomized trial evidence has not shown the same clear all-cause mortality reduction seen in coronary artery disease. The HF-ACTION trial, the largest randomized exercise trial in patients with heart failure with reduced ejection fraction, showed modest reductions in mortality and hospitalization that did not meet significance in the primary analysis, although adjusted analyses showed benefit for cardiovascular mortality or heart failure hospitalization.
But focusing only on mortality misses much of what matters to patients.
Exercise training in heart failure consistently improves functional capacity, exercise tolerance, and quality of life, and it reduces heart failure hospitalizations. A large retrospective cohort study of more than 40,000 propensity-matched patients found that exercise-based cardiac rehabilitation was associated with 42% lower odds of all-cause mortality at two years, with benefit observed in both HFrEF and HFpEF.
For a person with heart failure, the ability to walk farther, climb stairs, avoid hospitalization, and maintain independence is not a soft outcome. It is life itself.
COPD: movement predicts survival
COPD is often framed as a lung disease, but patients experience it as a disease of breathlessness, deconditioning, fear, muscle loss, and shrinking life space. Exercise directly targets that spiral.
The evidence document noted that physical activity is a strong predictor of mortality in COPD. A 2024 emulated target trial using nationwide cohort data found that initiating moderate-to-vigorous physical activity after COPD diagnosis was associated with a 16% reduction in all-cause mortality.
Population-based COPD data also show a dose-response relationship. Meeting physical activity guidelines was associated with lower all-cause mortality, cardiovascular mortality, and respiratory mortality compared with no physical activity. Importantly, benefits appeared even at levels below general recommendations.
Pulmonary rehabilitation after COPD hospitalization is one of the most practical examples of exercise as treatment. The GOLD guidelines state that pulmonary rehabilitation reduces mortality among patients hospitalized for acute exacerbations when started during hospitalization or within four weeks of discharge, and a Medicare study found that pulmonary rehabilitation initiated within 90 days of COPD hospitalization was associated with lower one-year mortality.
For COPD, exercise is not simply “fitness.” It is dyspnea management, muscle preservation, confidence rebuilding, hospitalization prevention, and survival strategy.
Cancer: the evidence has crossed a threshold
Cancer may be where the public most underestimates exercise.
A pan-cancer analysis of 11,480 cancer survivors found that exercise consistent with guidelines was associated with a 25% reduction in all-cause mortality compared with no exercise. A 2025 meta-analysis including nearly 1.5 million cancer patients confirmed survival benefits across multiple cancer types.
The most striking recent evidence comes from colon cancer. The 2025 CHALLENGE trial in the New England Journal of Medicine randomized 889 patients with resected colon cancer to a structured three-year exercise program after adjuvant chemotherapy or to health education materials. The structured exercise group had a 28% reduction in disease recurrence, new primary cancer, or death, and a 37% reduction in all-cause mortality. Five-year disease-free survival was 80.3% versus 73.9%, and eight-year overall survival was 90.3% versus 83.2%.
The authors noted that the magnitude of benefit from exercise after surgery and chemotherapy was similar to that of many currently approved standard drug treatments.
That sentence should stop us in our tracks.
If a pill produced a 37% mortality reduction after colon cancer treatment, it would be discussed at every oncology meeting, advertised to clinicians, and rapidly incorporated into care pathways. Exercise deserves the same seriousness.
Cancer-specific observational evidence also supports broad benefits. Physical activity after diagnosis has been associated with improved survival across breast, colorectal, prostate, lung, oral, endometrial, kidney, bladder, and other cancers. Even people who were inactive before diagnosis can benefit when they become active afterward.
It is not too late after diagnosis. It is not too late after treatment. The body can still respond.
The Bottom Line
If cardiorespiratory fitness is one of the strongest predictors of mortality, then exercise is the intervention that changes the predictor.
That is the central message.
Exercise is not merely a way to burn calories. It is not punishment for eating. It is not a hobby for athletes. It is a broad-spectrum medical intervention that improves the physiology underlying many chronic diseases at the same time.
It helps prevent disease. It helps treat disease. It improves quality of life while also improving survival in many high-risk groups. It is low cost, widely available, dose responsive, and adaptable to age, disability, diagnosis, and baseline fitness.
No single medication or screening test can make that claim across coronary artery disease, heart failure, COPD, cancer survivorship, diabetes risk, hypertension, frailty, depression, sleep, mobility, and all-cause mortality.
That does not mean exercise replaces medication, surgery, screening, rehabilitation, or medical care. It means exercise should be placed beside them, and often before them, as one of the most powerful interventions available.
The number your body knows is not a secret. It is being computed every time you climb stairs, walk across a parking lot, push up a hill, carry groceries, pedal a bike, or ask your breathing to deepen and your heart to work.
The question is whether we choose to pay attention to it.
Get Out & Move!
Reference List
Kokkinos P, Faselis C, Samuel I, et al. Cardiorespiratory Fitness and Mortality Risk Across the Spectra of Age, Race, and Sex. Journal of the American College of Cardiology. 2022;80(6):598-609. https://doi.org/10.1016/j.jacc.2022.05.031
Kokkinos P, Faselis C, Samuel I, et al. Changes in Cardiorespiratory Fitness and Survival in Patients With or Without Cardiovascular Disease. Journal of the American College of Cardiology. 2023;81(12):1137-1147. https://doi.org/10.1016/j.jacc.2023.01.027
Laukkanen JA, Isiuozor NM, Kunutsor SK. Objectively assessed cardiorespiratory fitness and all-cause mortality risk: an updated meta-analysis of 37 cohort studies involving 2,258,029 participants. Mayo Clinic Proceedings. 2022;97(6):1054-1073. https://doi.org/10.1016/j.mayocp.2022.02.029
Han M, Qie R, Shi X, et al. Cardiorespiratory fitness and mortality from all causes, cardiovascular disease and cancer: dose-response meta-analysis of cohort studies. British Journal of Sports Medicine. 2022;56(13):733-739. https://doi.org/10.1136/bjsports-2021-104876
Smart NA, Kwok S, Williams AD, Lyndon K, Dieberg G. Comparison of objectively measured and estimated cardiorespiratory fitness to predict all-cause and cardiovascular disease mortality in adults: a systematic review and meta-analysis of 42 studies representing 35 cohorts and 3.8 million observations. Journal of Sport and Health Science. 2024;13(5):642-651. https://doi.org/10.1016/j.jshs.2024.100986
Lang JJ, Prince SA, Merucci K, et al. Cardiorespiratory fitness is a strong and consistent predictor of morbidity and mortality among adults: an overview of meta-analyses representing over 20.9 million observations from 199 unique cohort studies. British Journal of Sports Medicine. 2024. https://doi.org/10.1136/bjsports-2023-107849
Vainshelboim B, Myers J, Matthews CE. Non-exercise estimated cardiorespiratory fitness and mortality from all-causes, cardiovascular disease, and cancer in the NIH-AARP Diet and Health Study. European Journal of Preventive Cardiology. 2022;29(4):599-607. https://doi.org/10.1093/eurjpc/zwaa131
Tucker WJ, Fegers-Wustrow I, Halle M, et al. Exercise for Primary and Secondary Prevention of Cardiovascular Disease: JACC Focus Seminar 1/4. Journal of the American College of Cardiology. 2022;80(11):1091-1106. https://pubmed.ncbi.nlm.nih.gov/36075680
Dibben GO, Faulkner J, Oldridge N, et al. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: A Meta-Analysis. European Heart Journal. 2023;44(6):452-469. https://pubmed.ncbi.nlm.nih.gov/36746187
Eijsvogels TMH, Maessen MFH, Bakker EA, et al. Association of Cardiac Rehabilitation With All-Cause Mortality Among Patients With Cardiovascular Disease in the Netherlands. JAMA Network Open. 2020;3(7):e2011686. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2020.11686
Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. Journal of the American College of Cardiology. 2022;79(17):e263-e421. https://doi.org/10.1016/j.jacc.2021.12.012
Buckley BJR, Harrison SL, Fazio-Eynullayeva E, et al. Cardiac Rehabilitation and All-Cause Mortality in Patients With Heart Failure: A Retrospective Cohort Study. European Journal of Preventive Cardiology. 2021;28(15):1704-1710. https://pubmed.ncbi.nlm.nih.gov/34333607
Global Initiative for Chronic Obstructive Lung Disease. 2026 GOLD Report: Global Strategy for Prevention, Diagnosis, and Management of COPD. https://goldcopd.org/wp-content/uploads/2026/01/GOLD-REPORT-2026-v1.3-8Dec2025_WMV2.pdf
Kim T, Kim H, Kong S, et al. Association Between Regular Moderate to Vigorous Physical Activity Initiation Following COPD Diagnosis and Mortality: An Emulated Target Trial Using Nationwide Cohort Data. Chest. 2024;165(1):84-94. https://pubmed.ncbi.nlm.nih.gov/37494977
Cheng SWM, McKeough Z, Alison J, et al. Associations of Total and Type-Specific Physical Activity With Mortality in Chronic Obstructive Pulmonary Disease: A Population-Based Cohort Study. BMC Public Health. 2018;18(1):268. https://pubmed.ncbi.nlm.nih.gov/29454345
Lindenauer PK, Stefan MS, Pekow PS, et al. Association Between Initiation of Pulmonary Rehabilitation After Hospitalization for COPD and 1-Year Survival Among Medicare Beneficiaries. JAMA. 2020;323(18):1813-1823. https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2020.4437
Lavery JA, Boutros PC, Scott JM, et al. Pan-Cancer Analysis of Postdiagnosis Exercise and Mortality. Journal of Clinical Oncology. 2023;41(32):4982-4992. https://pubmed.ncbi.nlm.nih.gov/37651670
Ungvari Z, Fekete M, Varga P, et al. Exercise and Survival Benefit in Cancer Patients: Evidence From a Comprehensive Meta-Analysis. GeroScience. 2025;47(3):5235-5255. https://pubmed.ncbi.nlm.nih.gov/40220151
Morishita S, Hamaue Y, Fukushima T, et al. Effect of Exercise on Mortality and Recurrence in Patients With Cancer: A Systematic Review and Meta-Analysis. Integrative Cancer Therapies. 2020;19:1534735420917462. https://pubmed.ncbi.nlm.nih.gov/32476493
Rees-Punia E, Teras LR, Newton CC, et al. Leisure-Time Physical Activity and Cancer Mortality Among Cancer Survivors. JAMA Network Open. 2026;9(2):e2556971. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2025.56971
Rees-Punia E, Teras LR, Newton CC, et al. Leisure-Time Physical Activity After Diagnosis and Survival by Cancer Type: A Pooled Analysis. Journal of the National Cancer Institute. 2025. https://pubmed.ncbi.nlm.nih.gov/40393661
Courneya KS, Vardy JL, O’Callaghan CJ, et al. Structured Exercise after Adjuvant Chemotherapy for Colon Cancer. New England Journal of Medicine. 2025;393(1):13-25. https://www.nejm.org/doi/full/10.1056/NEJMoa2502760
Schmid D, Leitzmann MF. Association Between Physical Activity and Mortality Among Breast Cancer and Colorectal Cancer Survivors: A Systematic Review and Meta-Analysis. Annals of Oncology. 2014;25(7):1293-1311. https://pubmed.ncbi.nlm.nih.gov/24644304
National Comprehensive Cancer Network. Survivorship Guidelines. https://www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf
Good Medscape article on topic by Dr Eric Topol https://www.medscape.com/s/viewarticle/flawed-v02-max-craze-2026a10007jm